INTEGRATIVE REVIEW
PRACTICES AND OPERATIONALIZATION OF WATER BIRTH: AN INTEGRATIVE REVIEW
PRÁTICAS E OPERACIONALIZAÇÃO DO PARTO AQUÁTICO: UMA REVISÃO INTEGRATIVA
PRÁCTICAS Y OPERACIONALIZACIÓN DEL PARTO EN AGUA: REVISIÓN INTEGRADORA
https://doi.org/10.31011/reaid-2026-v.100-n.2-art.2703
1Isabelle Souza Chies
2Júnia Aparecida Laia da Mata
3Clara Fróes de Oliveira Sanfelice
4Gabriela Capin Pagano
1Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, Rio Grande do Sul, Brazil. Orcid: https://orcid.org/0009-0000-2260-9755
2Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, Rio Grande do Sul, Brazil. Orcid: https://orcid.org/0000-0001-9062-8536
3Universidade Estadual de Campinas (Unicamp), Campinas, São Paulo, Brazil. Orcid: https://orcid.org/0000-0003-1920-3193
4Hospital de Clínicas e Porto Alegre (HCPA), Porto Alegre, Rio Grande do Sul, Brazil. Orcid: https://orcid.org/0000-0002-8287-4558
Corresponding Author
Júnia Aparecida Laia da Mata
Avenida Francisco Petuco, n. 45, apto 1004-B1, Boa Vista, Porto Alegre- RS, Brazil. CEP: 90.520-620, contato: +55(51) 99940-2505, E-mail: jumata.2905@gmail.com.
Submission: 05-12-2025
Approval: 15-04-2026
ABSTRACT
Introduction: Water birth is a strategy that promotes comfort, reduces interventions, and favors the physiology of birth. In Brazil, this practice is still not widespread and lacks specific guidelines, both in hospital settings and in planned home birth. Therefore, understanding how this modality is operationalized in different scenarios becomes essential to improving the quality of care. Objective: To understand water birth practices and their operationalization in Brazil and internationally, both in hospital and home settings. Method: An integrative literature review was conducted in six stages, guided by the PCC strategy and PRISMA-ScR recommendations. Searches were conducted in six national and international databases, including studies and documents published between 2013 and 2023. Results: The initial search identified 807 materials and, after screening and full reading, 18 comprised the final sample. The studies mainly addressed water birth in a hospital setting, with no publications on its implementation in planned home birth. The findings included eligibility criteria, care practices, water temperature control, maternal–fetal monitoring, hygiene aspects, and potential benefits and risks, including challenges in estimating blood loss. Conclusion: Water birth is an established practice in several countries but remains underexplored in Brazil. The lack of national studies and guidelines, especially for the home setting, highlights the need for scientific research to support safe and qualified practices.
Keywords: Water Birth; Natural Childbirth; Midwifery; Maternal Health.
RESUMO
Introdução: O parto aquático configura uma estratégia que promove conforto, reduz intervenções e favorece a fisiologia do nascimento. No Brasil, sua prática ainda é pouco difundida e carece de diretrizes específicas, tanto no contexto hospitalar quanto no parto domiciliar planejado. Diante disso, compreender como essa modalidade é operacionalizada em diferentes cenários torna-se essencial para qualificar a assistência. Objetivo: Conhecer as práticas de parto aquático e sua operacionalização no Brasil e no cenário internacional, tanto no ambiente hospitalar quanto no domiciliar. Método: Realizou-se uma revisão integrativa da literatura em seis etapas, orientada pela estratégia PCC e pelas recomendações PRISMA-ScR. As buscas foram conduzidas em seis bases de dados nacionais e internacionais, contemplando estudos e documentos publicados entre 2013 e 2023. Resultados: A busca inicial identificou 807 materiais e, após triagem e leitura na íntegra, 18 compuseram a amostra final. Os estudos abordaram majoritariamente o parto aquático em ambiente hospitalar, não havendo publicações sobre sua realização no parto domiciliar planejado. Os achados incluíram critérios de elegibilidade, práticas assistenciais, controle da temperatura da água, monitoramento materno-fetal, aspectos de higiene e potenciais benefícios e riscos, incluindo desafios na estimativa da perda sanguínea. Conclusão: O parto aquático é prática consolidada em diversos países, mas ainda pouco explorada no Brasil. A ausência de estudos e diretrizes nacionais, especialmente para o contexto domiciliar, evidencia a necessidade de produções científicas que subsidiem práticas seguras e qualificadas.
Palavras-chave: Parto na Água; Parto Humanizado; Enfermagem Obstétrica; Saúde Materna.
RESUMEN
Introducción: El parto en agua se configura como una estrategia que promueve confort, reduce intervenciones y favorece la fisiología del nacimiento. En Brasil, su práctica aún es poco difundida y carece de directrices específicas, tanto en el contexto hospitalario como en el parto domiciliario planificado. En este sentido, comprender cómo se operacionaliza esta modalidad en diferentes escenarios resulta esencial para calificar la atención. Objetivo: Conocer las prácticas de parto en agua y su operacionalización en Brasil y en el contexto internacional, tanto en el ámbito hospitalario como en el domiciliario. Método: Se realizó una revisión integradora de la literatura en seis etapas, guiada por la estrategia PCC y por las recomendaciones PRISMA-ScR. Las búsquedas se llevaron a cabo en seis bases de datos nacionales e internacionales, sobre la base de estudios y documentos publicados entre 2013 y 2023. Resultados: La búsqueda inicial identificó 807 materiales y, tras el proceso de selección y la lectura completa, 18 conformaron la muestra final. Los estudios abordaron mayoritariamente el parto en agua en el entorno hospitalario, sin haberse detectado publicaciones sobre su realización en el parto domiciliario planificado. Los hallazgos incluyeron criterios de elegibilidad, prácticas de atención, control de temperatura del agua, monitoreo materno-fetal, aspectos de higiene y posibles beneficios y riesgos, incluidos desafíos en la estimación de la pérdida sanguínea. Conclusión: El parto en agua es una práctica consolidada en diversos países, aunque aún poco explorada en Brasil. La ausencia de estudios y directrices nacionales, especialmente para el contexto domiciliario, evidencia la necesidad de producir investigaciones que respalden prácticas seguras y de calidad.
Palabras-clave: Parto en Agua; Parto Humanizado; Enfermería Obstétrica; Salud Materna.
INTRODUCTION
Physiological labor and delivery are defined as processes that begin and progress spontaneously at term, with the absence or minimal use of interventions and medications, resulting in an uncomplicated delivery, termed eutocic(1-2). Delivery of a low-risk pregnant woman can be assisted in a hospital setting and, in a planned home setting, by Obstetric Nurses and Midwives (3-5).
In Brazil, most births occur in hospitals, whereas planned home birth (PHB) remains limited to a minority segment of the population, generally attended in the private sector by specialized teams.
A systematic review with meta-analysis concluded that home birth PHB in women with usual risk pregnancies does not increase perinatal and neonatal mortality or morbidity when compared to women who intend to give birth in a hospital setting. Furthermore, when comparing home and hospital groups, no differences were observed in the following neonatal outcomes: admission to the Neonatal Intensive Care Unit (NICU), Apgar scores, and need for resuscitation(6).
Planned home birth is as safe as hospital birth when it comes to the care of pregnant women stratified as usual risk(3), and it is possible for it to take place in an aquatic environment. However, in Brazil, there is a lack of specific guidelines for the operationalization of water birth, which may compromise the quality and safety of care.
The World Health Organization (WHO), since 1996, has recommended offering childbirth and delivery assistance where the pregnant woman chooses, feels comfortable, and where the birth is feasible(7). Promoting the physiology of birth involves reducing the routine use of unnecessary interventions and includes adopting practices that facilitate psychological and physical aspects during the process. Among these, we highlight water immersion, recommended for promoting comfort and pain relief(8-11).
Scientific research demonstrates that immersion in water during labor promotes physiology(10,11), provides a person-centered experience for the mother,(12,13) reduces pain and increases maternal satisfaction(8-10,13-16). In addition to these benefits, immersion in warm water, in a bathtub or pool, reduces the incidence of perineal trauma during birth, promotes relaxation, enables freedom of movement, and ensures safety for both mother and fetus(17).
The first historical mention of the concept of water birth occurred in 1805 in France, in the mid-1960s, by researchers Tscharkowskij and Frédérick Leboyer. The first reported record of a water birth, however, only occurred in 1980 in the United States of America, being called a "water baby", taking place in a bathtub at home(18). In 1983, Michel Odent, an obstetrician and a reference in the humanization of childbirth, published his research conducted with 100 women who experienced water birth, being a pioneer in this practice(19).
Currently, immersion in water during labor and birth is recommended by the WHO and the Ministry of Health(8,15). Water birth is a great example in which power relations in childbirth are reversed: the person giving birth leads the process, while the professional assisting them focuses on care (20). Perhaps for this reason, it is common to find, on the internet, photographic records of water births at home, a context in which pregnant women and their families frequently seek and find greater autonomy to experience the birthing process.
Given the above and considering the importance of understanding the operational aspects of water birth in different birth modalities, this study was developed with the objective of understanding water birth practices and their implementation in Brazil and internationally, both in hospital and home settings.
METHOD
This was an integrative literature review (ILR), developed in six steps: 1) definition of the theme and selection of the research question, which sought to understand aquatic birth practices in Brazil and internationally, to promote reflection on the possibility of adopting them in childbirth care; 2) establishment of inclusion and exclusion criteria for the materials; 3) identification of pre-selected and selected studies; 4) categorization of studies; 5) analysis and interpretation of results; and, 6) presentation of a synthesis of the knowledge(21,22).
The question for this ILR was constructed using the PCC (Population, Concept, Context) strategy, as proposed by the recommendations of the Joanna Briggs Institute (JBI)(23), and considered: population - low-risk pregnant women; concept - water birth; and context – Brazilian and international scope. Thus, the following question was obtained: What are the water birth practices for low-risk pregnant women in Brazil and internationally, as described in the scientific literature?
Data collection was carried out between June and August 2023, using the following databases: Cochrane; Scopus; Science Direct; Biomed Central; Latin American and Caribbean Health Sciences Literature (LILACS) and Medical Literature Analysis and Retrieval System Online (MEDLINE), the latter two accessed through the Virtual Health Library (VHL). Original research, guidelines, manuals/guidelines, legislation, technical notes, protocols, theses, dissertations, and national and international consensus statements were included; published between 2013 and 2023, nationally and internationally, in Portuguese, English, and Spanish. Integrative review articles, articles addressing water birth in high-risk pregnancies, and materials that did not answer the question of this ILR were excluded.
The search process was developed using Health Sciences Descriptors (DeCS) in Portuguese, English, and Spanish, and Medical Subject Headings (MeSH), combined using the Boolean operators AND, OR, or NOT, as shown in Chart 1. The development of data collection strategies was carried out with the support of a librarian with experience in supporting studies in the field of health sciences.
Chart 1 – ILR's search strategies in Portuguese, English, and Spanish. Porto alegre, 2025.
|
Search in Portuguese |
Search in English |
Search in Spanish |
|
("parto natural" OR "parto em casa" OR parto na água) AND água NOT dor. |
("natural childbirth" OR "home childbirth" OR "water birth" OR waterbirth) AND water NOT pain.
|
("parto natural" OR "parto en casa" OR parto en el agua) AND agua NOT dolor.
|
Source: Prepared by the authors, 2025.
Prior to this ILR, an exploratory search was conducted in the databases and, although many studies addressing the practice of water immersion were identified, in most of them, childbirth/birth did not occur in an aquatic environment, the main focus of this study. The materials centered on pain management. Therefore, we opted to use "NOT pain" in the search strategy.
In the pre-selection process, the titles and abstracts/descriptions/presentations of the materials were analyzed, and those that met the inclusion criteria were selected and analyzed in full. Materials indexed in more than one database were counted only once.
The selection of materials involved two researchers, and the data extraction was recorded in an Excel® spreadsheet containing the following information: title, authors, year, type of study/material, country of publication, and main research findings. Rayyan® was used to filter the materials.
In this ILR, the PRISMA Extension for Scoping Reviews (PRISMA-ScR) initiative was followed(24), with the study selection process presented in the results. To synthesize the findings, a chart with the main characteristics of the studies was prepared, aiming to present an overview of all the material. In addition to the numerical presentation of the results, a thematic description was organized and presented.
In accordance with research regulations and Copyright Law number 9.610 of February 19, 1998(25), all data identified in the literature were duly referenced with respect to ethical rigor and intellectual property.
RESULTS
This ILR sample resulted in 19 materials. The entire selection process, based on PRISMA-ScR, is shown in Figure 1.
Figure 1 - ILR flowchart based on the PRISMA Extension for Scoping Reviews (PRISMA-ScR). Porto Alegre, 2025.
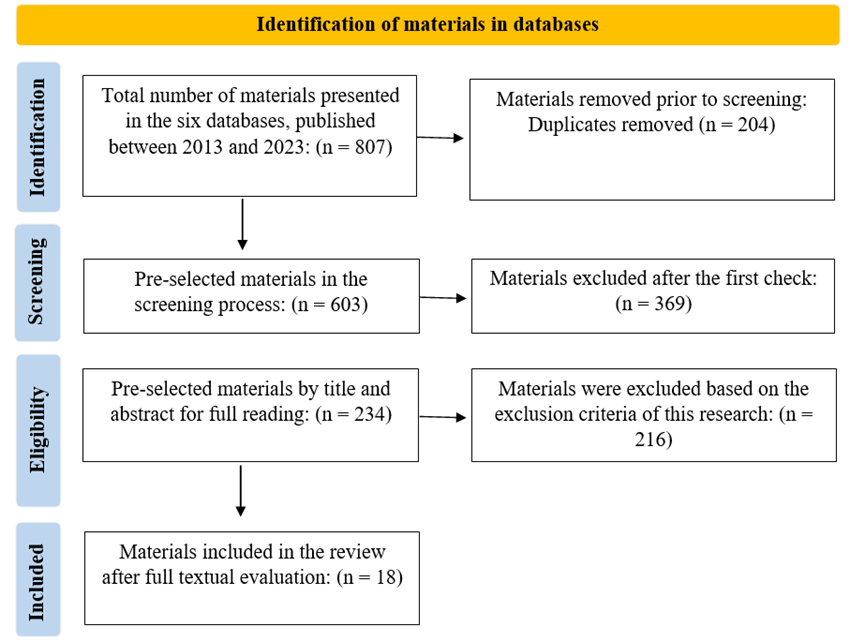
Source: Prepared by the authors, 2025.
Of the selected studies, four were published in Australia, three in the United States of America, two in Turkey, two in Italy, and one article each from the remaining countries (Chart 2). Of these, 13 were quantitative, and 6 were qualitative.
The English language prevailed in the included materials. All address the effects of water birth on maternal and neonatal health in a hospital setting. No studies were found that dealt with water birth in PHB, even though this scenario was also part of the scope of this ILR. No Brazilian research was identified in the databases investigated. Chart 2 presents the characterization of the included materials.
Chart 2 – Coding and characterization of materials according to author(s), title, objective(s), type of study/method, publisher/journal, country of origin, and year of publication. Porto Alegre, Rio Grande do Sul, Brazil, 2025.
|
Code and Author(s)
|
Title |
Objective(s) |
Type/Method |
Publisher/Journal and Country of Origin |
Year of Publication |
|
A1
LIM, K. et al. (26) |
A comparative study between the pioneer cohort of waterbirths and conventional vaginal deliveries in an obstetrician led unit in Singapore. |
To evaluate whether water immersion during childbirth is associated with increased rates of adverse maternal and fetal outcomes compared to conventional vaginal deliveries. |
Cohort study analyzing women who gave birth underwater at a national university hospital between 2010 and 2013. |
Taiwanese Journal of Obstetrics and Gynecology.
Singapore. |
2016 |
|
A2
KAVOSI, Z. et al.(27) |
A Comparison of Mothers' Quality of Life (QV) after Normal Vaginal, Cesarean, and Water Birth Deliveries. |
To evaluate and compare postpartum quality of life (QoL) after cesarean section (CS), normal vaginal delivery (NVD), and water birth. |
This descriptive, analytical, and cross-sectional study was conducted on postpartum women referred to urban health centers and two public hospitals in 2012-2013 in Shiraz, Iran. Data were analyzed using descriptive statistics and one-way analysis of variance (ANOVA) in SPSS version 18. |
International Journal of Community Based Nursing and Midwifery.
Iran. |
2015 |
|
A3
COOPER, M. et al.(28) |
A critical analysis of Australian policies and guidelines for water immersion during labour and birth. |
To determine how water immersion policies and/or guidelines are communicated, and to what extent these facilitate the choice of labor and delivery. |
First phase of a three-phase mixed-methods study that critically analyzed 25 Australian water immersion policies/guidelines using critical discourse analysis. |
Women and Birth.
Australia. |
2017 |
|
A4
SEED, E. et al.(29) |
A prospective cohort study comparing neonatal outcomes of waterbirth and land birth in an Australian tertiary maternity unit. |
To investigate the maternal and neonatal outcomes after water immersion in the first stage of labor and/or water birth compared to birth outside of water. |
A prospective cohort study was conducted at an Australian public maternity hospital between 2019 and 2020. Maternal and neonatal outcomes of 1,665 women who had vaginal deliveries were studied. |
Australian and New Zealand Journal of Obstetrics and Gynaecology.
Australia. |
2022 |
|
A5
MENAKAYA, U. et al.(30) |
A retrospective comparison of water birth and conventional vaginal birth among women deemed to be low risk in a secondary level hospital in Australia. |
To describe the maternal and neonatal outcomes associated with water birth among women in labor considered low risk for obstetric complications and compare these outcomes with women of similar risk who had a standard out-of-water birth. |
A retrospective and comparative audit of women who gave birth in water with a matching cut, who were born at Bankstown Hospital, over a 10-year period (2000–2009). |
Women and Birth.
Australia. |
2013 |
|
A6
HARPER, B.(31) |
Birth, bath, and beyond: the science and safety of water immersion during labor and birth. |
To explain the physiology of the newborn and the protective mechanisms that prevent babies from breathing during water birth. |
This article provides a retrospective literature review on water birth. |
The Journal of Perinatal Education.
United States of America. |
2014 |
|
A7
BURNS, E. et al.(32) |
Developing and evaluating an online learning tool to improve Midwives’ accuracy of visual estimation of blood loss during waterbirth: An experimental study. |
The main objective was to test the effectiveness of an online learning tool to improve the accuracy of Midwives in estimating blood loss in a delivery pool environment. |
Experimental study with Midwives who had experience caring for pregnant women. |
Midwifery.
United Kingdom. |
2019 |
|
A8
MAUDE, R.M.; KIM, M. (33) |
Getting into the water: A prospective observational study of water immersion for labour and birth at a New Zealand District Health Board (DHB). |
To describe the maternal characteristics, intrapartum events, interventions, and neonatal outcomes of women who used water during labor and delivery at the District Health Council in New Zealand. |
This article presents the results of a prospective observational study of women who used water immersion for labor and delivery in three maternity hospitals, from February 2009 to March 2014. |
BMC Pregnancy and Childbirth.
New Zealand. |
2020 |
|
A9
HENDERSON, J. et al. (34) |
Labouring women who used a birthing pool in obstetric units in Italy: prospective observational study. |
To describe and compare maternal characteristics, intrapartum events, interventions, and maternal and neonatal outcomes for all women who used a birthing pool. |
An observational, prospective study conducted in 19 Italian obstetric units between 2002 and 2005. Descriptive statistics were calculated and compared using Chi-square statistics and continuous data by t-tests. |
BMC Pregnancy and Childbirth.
Italy. |
2014 |
|
A10
ULFSDOTTIR, H. et al.(35) |
Management of the active second stage of labor in waterbirths compared with conventional births - a prospective cohort study. |
To describe how midwives manage the second active phase of labor in water births in comparison with conventional births and compare the results between the two groups. |
A prospective cohort study, based on 323 women who gave birth at three clinics in Sweden between December 2015 and May 2019. |
Midwifery.
Sweden. |
2022 |
|
A11
UCCELLA, S. et al.(36) |
Neonatal Outcomes of Water Delivery versus Land Delivery: A Retrospective Propensity Score Weighted Study. |
To contribute to the available evidence on maternal and neonatal outcomes associated with water provision. |
A retrospective cohort study based on birth registry data prospectively collected from 2015 to 2019. The inverse probability of treatment weighting (IPTW) method was applied to address confounding factors. |
American Journal of Perinatology.
Italy. |
2023 |
|
A12
LEWIS, L. et al.(37) |
Obstetric and neonatal outcomes for women intending to use immersion in water forlabour and birth in Western Australia (2015-2016): A retrospective audit of clinical outcomes. |
To evaluate the obstetric and neonatal outcomes of women who intend to use water immersion during labor or delivery. |
A retrospective audit of clinical outcomes for women intending to have labor or give birth in water, conducted between July 2015 and June 2016, at a tertiary maternity center in Western Australia. |
Australian and New Zealand Journal of Obstetrics and Gynaecology.
Australia. |
2018 |
|
A13
BASHAIKH, S.M.; MAHBOUB, F.A.; ORABI, A.(38) |
Perception and knowledge of Saudi women about water birth: A cross sectional study. |
To evaluate the perception and knowledge of Saudi women regarding water birth. |
A cross-sectional study was conducted with 388 Saudi women. Data collection was carried out using an online questionnaire that included four sections: sociodemographic characteristics, obstetric history, perception and knowledge about water birth. Descriptive statistics and inferential statistics (Chi-square, Fisher's exact test, and t-tests) were used for data analysis. |
Belitung Nursing Journal.
Saudi Arabia. |
2022 |
|
A14
CAMARGO, J. et al.(39) |
Perineal outcomes and its associated variables of water births versus non water births: a cross-sectional study. |
To describe the perineal outcomes of women who gave birth in water and outside of water. |
This cross-sectional and quantitative study was conducted in a public hospital in Setúbal, Portugal. The population consisted of women who participated in the "Projeto Parto na Água" (Water Birth Project), between 2011 and 2014, who gave birth both in and out of water. Data were analyzed using Stata(r), software, with descriptive and bivariate statistics (Chi-square and Fisher's exact test). |
Revista Brasileira de Saúde Materno-Infantil.
Portugal. |
2019 |
|
A15
YORGANCI, A. et al.(40) |
The effects of water immersion during first stage of labor on postpartum systemic inflammatory response. |
To determine the effects of water immersion during the first stage of labor on systemic inflammatory indices in the postpartum period. |
In this retrospective study, 125 healthy multiparous women who chose water immersion during the first stage of labor were compared with term multiparous women without complications who had conventional vaginal births out of water. |
Thieme.
Turkey. |
2021 |
|
A16
WEAVER, MH.(18) |
Water birth in the hospital setting. |
To provide information for professionals, to support guidance and informed decisions about water birth. |
Recommendations for professionals. |
Nursing for Women's Health.
United States of America. |
2014 |
|
A17
SERT, U.Y. et al.(41)
|
Water Immersion During the Labour and Effects on Oxidative Stress. |
To investigate maternal serum thiol/disulfide levels and ischemia-modified albumin (IMA) levels in women who remained immersed during labor. |
A prospective, randomized, and controlled study. Sixty-four pregnant women were included. |
Fetal and Pediatric Pathology.
Turkey. |
2020 |
|
A18
NUTTER, E.; SHAW BATTISTA, J; MAROWITZ, A.(42) |
Waterbirth fundamentals for clinicians. |
To present a combination of general physiological principles and specific practical recommendations to facilitate safety during water birth. |
Na integrative analysis with 38 peer-reviewed studies. |
Journal of Midwifery & Women’s Health Resources for Clinicians.
United States of Ameria. |
2014 |
DISCUSSION
Indications and contraindications for water birth
Water birth is indicated for specific situations and involves the following eligibility criteria: low-risk pregnancy; singleton pregnancy >37 weeks; cephalic presentation; clear amniotic fluid; and normal fetal heart rate monitoring. In circumstances with the presence of meconium, labor can occur in the bathtub, however, the expulsion of the baby must take place outside the aquatic environment(18).
Water birth is contraindicated in the following situations: premature labor (<37 weeks gestation); transmissible maternal infections (hepatitis and syphilis); severe intrauterine growth restriction; maternal fever; excessive vaginal bleeding; indeterminate fetal heart rate tracking and conditions requiring close intrapartum monitoring (severe pre-eclampsia and diabetes); suspected macrosomia with a history of shoulder dystocia (labor can be performed in a bathtub/pool, however, delivery outside of it is necessary); two or more previous cesarean sections; fetal malpresentation; and multiple births(18,26).
Criteria and practices for offering water birth
Water birth can take place in a pool or bathtub, ideally large enough to allow the person giving birth to adopt any position. Furthermore, the depth should allow for complete immersion, but not be excessively great, as this requires a long time to fill and empty(19).
According to Michel Odent, a round pool, approximately 2 meters in diameter and 70 centimeters deep, is the perfect model. The predominant colors should be taken into account, considering that blue light promotes an aquatic atmosphere(19).
Water immersion can occur throughout labor and postpartum without complications. During labor, the water temperature should be around 37ºC, and the mother's stay in the water should not be too long, as relaxation can become detrimental to fetal vitality and maternal-fetal circulation, causing unnecessary strain and overload for both mother and fetus(43).
According to Enning(43), ideally the mother's abdomen should be covered by water, with the bathtub/pool being at least 50 cm high. In water, the pelvic floor and vaginal walls offer relatively little resistance, as it promotes increased tissue elasticity. Four articles (A1, A5, A9, and A12) recommended that the water level should be at the level of the breasts and armpits. To date, there is no scientific evidence that different degrees of immersion or the amount of mobility possible within the bathtub/pool affect maternal-neonatal outcomes(44).
It is known that water temperature is an important factor in immersion care during labor, and the scientific literature presents a variety of suitable temperatures. The only consensus is that the water temperature should not exceed 38°C, due to the risk of fetal hyperthermia caused by elevated maternal temperatures, which could result in cerebral vasodilation and increased oxygen consumption, leading to fetal hypoxia(42).
Data on the use of water immersion in labor and delivery are limited, but most scientists suggest the ideal temperature is between 36 and 37.5°C, appearing in ten articles (A1, A5, A6, A8, A11, A14, A15, A16, A17, A18). This temperature is considered ideal to avoid hyperthermia and the risk of premature breathing during underwater delivery(45). Only one manuscript (A8) addressed the water temperature when the participant left the tub, which varied between 24°C and 42°C, maintaining an average of 36.7°C(33).
The guideline entitled Labour and/or Birth Using Water, from King Edward Memorial Hospital(46), of the Australian government, indicates that immersion in water in a bathtub/pool during the first stage of labor reduces the need for pain relief medication, making the experience more pleasant for the mother. There are so-called “corner bathtubs”, which provide greater ease in changing positions during labor. These are widely used, especially in Europe, where there is an infrastructure for water birth in clinics(35).
There is controversy regarding water hygiene. In a cohort study conducted in Singapore, hygiene was maintained throughout labor, with fecal matter removed (using sieves) and water changes performed. Professionals used long, sterile gloves as personal protective equipment (PPE)(26).
Only three selected articles (A1, A5, and A12) explained pool hygiene, and these encourage getting out of the bathtub to urinate. Only regular tap water should be used to fill the pool/bathtub, without the addition of substances (such as essential oils, for example)(37).
The Brazilian Ministry of Health's National Guidelines for Normal Childbirth Assistance indicate that none of the reference materials consulted for water births addressed specific aseptic and hygiene measures, including those related to the bathtub(15).
In two studies (A1 and A12), the newborn was immediately brought to the surface of the water after delivery and, in cases of fetal or maternal compromise, the women were immediately removed from the aquatic environment and attended to according to the safety protocol(26,37). This method of assisting aquatic childbirth demonstrated a smoother transition for the newborn and, therefore, it was argued that it should be offered to women with low-risk pregnancies(26).
Regarding the monitoring of maternal vital signs, research showed a consensus on a frequency of 15-30 minutes. Five articles (A1, A11, A15, A16, and A18) advocated for the measurement of maternal and fetal vital signs using cardiotocography (CTG). In this case, CTG can be performed at 30-minute intervals in the first stage of labor and after each contraction, or at least every 5 to 15 minutes.
In the second stage of labor, a waterproof Doppler ultrasound or telemetry unit is used. If there are changes in fetal heart rate, changes in maternal position, and intrauterine resuscitation in water may be applied(18,40,42).
Five articles (A8, A9, A11, A12, and A14) analyzed cervical dilation upon entering the pool/bathtub. Most participants presented with a dilation of 5 cm, and it was unanimous that they entered with a cervical dilation greater than or equal to 4 cm. A study that aimed to describe maternal characteristics in aquatic birth found no relationship between cervical dilation upon entering the pool and the duration of labor. Individualized care in aquatic birth should be considered when determining the appropriate time to enter the tub or pool(34).
After the birth of the newborn, the bathtub/pool must be drained and disinfected, including the hoses used. The expulsion of the placenta and amniotic membranes (placental delivery or afterbirth) occurs outside the bathtub to avoid potential risks of water embolism and to allow adequate evaluation of blood loss. After the expulsive phase, the individual may also leave the bathtub with the newborn still attached via the umbilical cord and subsequently experience placental delivery outside the water(30).
Physiological theory holds that the newborn should be born completely submerged, without exposure to colder temperatures or air, until its face is brought to the surface of the water. In water birth, the newborn should be gently guided to the surface within 5 to 10 seconds. The exposed head should be dried to minimize heat loss, and immediate skin-to-skin contact should be implemented(12).
There have been reports of neonatal infection with Legionella pneumophila and Pseudomonas aeruginosa when established protocols for water birth were not followed or when contaminated water was used(29). Thus, water quality can be considered a significant factor in the provision of this type of care.
Possible outcomes of water birth
Childbirth is a physiological and multidimensional process involving physical, psychological, and cultural aspects. Scientific research has shown that women who experienced water birth had the highest average total quality of life scores compared to postpartum women who had vaginal births outside of an aquatic environment or cesarean sections(27).
The challenges of practicing water birth include the risk of neonatal aspiration, possible drowning, umbilical cord prolapse, and potentially increased rates of maternal and neonatal infections. Commonly, the presence of a obstetric nurse or midwife is fundamental in this type of birth, reinforcing the mother's role of autonomy and power of choice(28).
Studies indicate that the person giving birth should leave the pool/bathtub during the third stage of labor (placental delivery or afterbirth) due to difficulties in estimating blood loss. Others have demonstrated a decrease in blood loss during water birth, resulting from muscle relaxation and improved blood circulation(32,36). Given this ambiguity, it is important to emphasize once again the importance of providing individualized care during water births, taking into account the mother’s, the fetus’s, the family’s, and the facility’s conditions.
In the postpartum period, two methods can be chosen: 1) the warm water method, which will keep the placenta functioning for some time; however, the mother must get out of the water to expel the placenta outside the bathtub, to prevent water and germs from entering the bloodstream(17).
Warm water induces local vasodilation, leading to increased regional tissue metabolism, tissue temperature, nerve conduction velocity, and muscle relaxation; comfort reduces anxiety and decreases the production of stress-related hormones, such as catecholamines and norepinephrine; (2) the Tscharkowskij method (cold-water immersion), in which the temperature is maintained at approximately 30°C, producing vasoconstriction of the vessel walls and thereby substantially reducing the risk of postpartum hemorrhage(17).
In fact, the scientific research used in this study demonstrates that immersion in warm water and water birth result in greater maternal satisfaction with the birthing experience, precisely because the person giving birth has a greater sense of control during the labor process.
A Cochrane systematic review demonstrated that the hydrothermal characteristics of water can offer protection against major perineal trauma(30). However, issues such as the risk of infection for mother and baby, water inhalation by the neonate, and the limited evidence on how to manage the third stage of labor in water remain important concerns for opponents of water birth.
Literature shows that there are several mechanisms that prevent a baby from breathing in or choking while still submerged in water. When the baby transitions from fetal to postnatal circulation, one of the main factors stimulating breathing is the influence of gravity, which acts uniformly on the face and stimulates the innervation of the trigeminal nerve (fifth cranial nerve) around the nose and mouth. To initiate the change from fetal to neonatal circulation, humans require both gravitational force and the presence of oxygen and carbon dioxide molecules(47).
Physiologist and researcher Paul Johnson from the University of Oxford states that the presence of fluid in the alveolar spaces of the lungs during the prenatal period is one of several inhibitory factors that prevent the baby from choking or breathing when briefly exposed to water during a water birth(28).
The risk of infection during water birth is one of the most concerning factors in the process. Rosenthal was remarkably ahead of his time in emphasizing that "the solution to pollution is dilution". He studied the technique of water dilution, which proved effective in reducing exposure to potentially harmful bacteria. It has already been clarified that every baby needs contact with the microorganisms present in the mother's vagina and rectum to develop adequate microbial protection (personal microbiota)(47).
Studies investigating the presence of Group B Streptococcus in aquatic newborns have shown a tendency toward lower bacterial colonization in babies born in water compared to those born outside of it(47). Therefore, concerns about harm to the baby from contamination are lessened, and the focus can shift to the potential benefits of water birth for maternal and child health.
Individuals who test positive for Group B Streptococcus and those whose amniotic membranes have been ruptured for more than 18 hours may use water immersion during labor and delivery, provided they follow the recommended antibiotic regimen(37). Three articles (A6, A12, and A17) presented results on the incidence of neonatal infections, revealing reports of Legionella pneumophila and Pseudomonas aeruginosa infections resulting from deviations from established water birth protocols or the use of impure water. Specifically regarding the water used, no increased infection rates were identified, either maternal or neonatal.
Implementing infection control policies is essential in all birthing settings to prevent the incidence of serious infections. Considering the use of birthing pools and multi-use birthing equipment, the key aspect in preventing infections and cross-contamination is the adoption of disposable or easily washable items(31).
Another important factor in the birthing process is blood loss. This amount varies considerably from person to person in the first 24 hours after delivery. Visual evaluation of the quantity and rate of blood loss provides a starting point for initial monitoring of maternal well-being.
During pregnancy, circulating blood volume increases to approximately 100 ml/kg of the pregnant person's weight. Currently, increasingly technological tools are being developed to measure blood loss. This includes clinical simulations that use known quantities of blood applied to objects, allowing for a precise comparison between gravimetric measurement of blood loss and visual estimates. However, this approach faces challenges due to the imprecise nature of measurement, as it is an inexact science(32).
Although measuring shock during aquatic births is challenging, professionals can also examine the person for signs and symptoms of shock, such as feeling faint or dizzy, paleness and clammy skin, low blood pressure, and increased heart and respiratory rate(48). In addition to clinical evaluation, the use of the shock index is recommended as an additional parameter for the early identification of hemodynamic instability. The shock index, calculated as the ratio between heart rate and systolic blood pressure, has proven to be a simple, sensitive, and safer measure for detecting early signs of hemorrhagic shock, including in obstetric settings. Elevated values suggest worsening perfusion and the possibility of clinical deterioration, allowing professionals to adopt timely interventions, especially in situations where direct measurement of blood loss is difficult, such as in water births.
Regarding the risk of obstetric emergencies, based on the study by Stefano Uccella and colleagues(36), it was inferred that the difference in temperature and osmotic pressure around the umbilical cord during labor in water immersion may be related to the occurrence of cord prolapse.
When the umbilical cord is exposed to water at 37°C, it can physiologically avoid vasoconstriction caused by lower temperatures, which would normally lead to physiological occlusion of the umbilical vessels. This, in turn, can negatively impact its resistance, increasing the likelihood of prolapse(36).
In water birth assistance, it is important to consider that systemic opioids have the potential to suppress the fetal diving reflex, increasing the risk of water aspiration by the fetus; therefore, their use is not advisable in this birth environment(12).
As for well-being, the buoyancy of water gives a person a feeling of lightness, allowing them to move more easily than they would on land(40).
It is worth noting that during the Covid-19 pandemic, the practice of water birth was discouraged due to the risk of transmitting the virus to the baby or the midwife during labor, through infected feces and maternal blood, which can contaminate the water in the pool/bathtub(49). At the time, it was recommended that women in labor leave the water for fetal evaluation and that the birth not take place in the water.
In summary, the materials gathered from the databases and those that supported this discussion present experiences and recommendations related to equipment for providing water birth, the need for water temperature control, maternal and fetal monitoring for the prevention of harm, individualized care, and hygiene practices focused on the prevention of maternal and neonatal infections.
In Brazil, water birth is not a standardized practice in the hospital setting. It occurs more frequently in the PHB, offered mainly by Obstetric Nurses and Midwives(3). Therefore, it is essential to know the criteria and recommendations for ensuring the quality and safety of maternal and infant care.
Although no materials addressing water birth at home were identified in the databases, many of the recommendations found can guide the care provided by nurses and midwives attending both PHB and hospital births. This result also reveals the need for research focusing on births that occur outside of hospital settings. Studies also demonstrate a clear need for more information and education about this type of birth from society(38).
FINAL CONSIDERATIONS
This review indicated that the scientific literature focuses on approaches to water birth in hospital settings, with no publications found on the implementation of this practice in planned home-birth contexts.
In certain countries, such as the United Kingdom and Australia, water birth is integrated into routine care, with birthing tubs or pools properly installed in hospital settings.
Regarding international practices related to water birth and its implementation, identified in this review, there is consensus on fundamental aspects of care: maintaining adequate hygiene of pools/bathtubs and equipment used; controlling the water temperature to around 37°C; continuous monitoring of maternal vital signs and fetal well-being; submerging the parturient up to the level of her breasts; ensuring clean water, with proper management of bodily fluids eliminated during labor or changing the water when necessary; encouraging free movement and postural freedom within the pool/bathtub; and careful attention to the placental delivery period, with a view to preventing hemorrhagic complications.
In Brazil, the practice of water birth is not widely available within the Unified Health System (SUS), and is therefore more frequently publicized on social media and digital platforms in a home setting, generally performed by private teams. This scenario, however, contrasts sharply with the scarcity of national guidelines, institutional protocols, and scientific evidence produced in the country regarding the safety, eligibility criteria, and operationalization of this type of care.
Given this, it is essential to develop research that deepens the understanding of water birth in different care contexts, contributing to improving practice, guiding professionals, and supporting the formulation of evidence-based public policies. The lack of national scientific publications represents an obstacle to the safe and qualified practice of professionals providing care, and may compromise the proper and safe implementation of this type of birth.
It is understood that the international recommendations presented in this research can be applied in both hospital and home settings. However, the importance of developing specific studies on water birth at home in the Brazilian context is highlighted, in order to broaden the understanding of its particularities and evaluate the maternal and neonatal outcomes associated with this type of care.
REFERENCES
1. American College of Nurse-Midwives, Midwives Alliance of North America, National Association of Certified Professional Midwives. Supporting healthy and normal physiologic childbirth: a consensus statement. J Midwifery Womens Health. 2012 Sep;57(5):529-32. doi:10.1111/j.1542-2011.2012.00218.x
2. Maternity Care Working Party. Making normal birth a reality: consensus statement from the Maternity Care Working Party: our shared views about the need to recognise, facilitate and audit normal birth [Internet]. London: National Childbirth Trust; Royal College of Midwives; Royal College of Obstetricians and Gynaecologists; 2007 [citado 2022 Set 23]. Disponível em: https://bhpelopartonormal.pbh.gov.br/estudos_cientificos/arquivos/normal_birth_consensus.pdf
3. Mata JAL. Enfermagem obstétrica no parto domiciliar planejado: responsabilidade legal e organização do serviço. In: Morais SCRV, Souza KV, Duarte ED, organizadoras. PROENF: Programa de Atualização em Enfermagem: Saúde Materna e Neonatal. Porto Alegre: Artmed Panamericana; 2017. p. 75–125. (Sistema de Educação Continuada a Distância; v. 4).
4. Conselho Regional de Enfermagem do Paraná. Parecer Técnico nº 001/2016. Atuação de Enfermeiro Obstétrico que assiste ao parto domiciliar e critérios para cadastramento para fins de emissão e preenchimento de Declaração de Nascido Vivo [Internet]. Curitiba: COREN-PR; 2016 [citado 2024 Ago 16]. Disponível em: https://www.corenpr.gov.br/portal/images/pareceres/PARTEC_16-001-Atuacao_enfermeiro_obstetrico_parto_domiciliar_declaracao_nascido_vivo.pdf
5. Conselho Regional de Enfermagem de Santa Catarina. Parecer Técnico COREN/SC nº 023/CT/2016. Parto domiciliar planejado [Internet]. Florianópolis: COREN-SC; 2016 [citado 2024 ago 16]. Disponível em: http://www.corensc.gov.br/wp-content/uploads/2017/01/PT-023-2016-Parto-DomiciliarPlanejado.pdf
6. Hutton EK, Reitsma A, Simioni J, Brunton G, Kaufman K. Perinatal or neonatal mortality among women who intend to give birth at home compared with women of low obstetrical risk who intend hospital birth: systematic review and meta-analyses. EClinicalMedicine. 2019 Sep;14:59–70. doi:10.1016/j.eclinm.2019.07.005
7. Santos LM, Mata JAL, Vaccari A, Sanfelice CFO. Trajectories of obstetric nurses in the care of planned home childbirth: oral history. Rev Gaúcha Enferm. 2021;42(spe):e20200185. doi:10.1590/1983-1447.2021.20200185.
8. World Health Organization. WHO recommendations: intrapartum care for a positive childbirth experience [Internet]. Geneva: WHO; 2018 [citado 2024 Ago 16]. Disponível em: https://www.who.int/publications/i/item/9789241550215
9. Carpenter J, Burns E, Smith L. Factors associated with normal physiologic birth for women who labor in water: a secondary analysis of a prospective observational study. J Midwifery Womens Health. 2022;67(1):13-20. doi:10.1111/jmwh.13315
10. Shaw-Battista J. Systematic review of hydrotherapy research. J Perinat Neonatal Nurs. 2017 Oct;31(4):303-16. doi:10.1097/JPN.0000000000000260
11. Liu Y, Li S, Tang Y, Wang L, Zhang W. A comparison of maternal and neonatal outcomes between water immersion during labor and conventional labor and delivery. BMC Pregnancy Childbirth. 2014 May;14:160. doi:10.1186/1471-2393-14-160
12. Nutter E, Meyer S, Shaw-Battista J, Marowitz A. Waterbirth: an integrative analysis of peer-reviewed literature. J Midwifery Womens Health. 2014 May;59(3):286-319. doi:10.1111/jmwh.12194
13. Burns EE, Boulton MG, Cluett E, Cornelius VR, Smith LA. Characteristics, interventions, and outcomes of women who used a birthing pool: a prospective observational study. Birth. 2012 Sep;39(3):192-202. doi:10.1111/j.1523-536X.2012.00548.x
14. Feeley C, Cooper M, Burns E. A systematic meta-thematic synthesis to examine the views and experiences of women following water immersion during labour and waterbirth. J Adv Nurs. 2021 Jul;77(7):2942-56. doi:10.1111/jan.14720
15. Ministério da Saúde (BR). Comissão Nacional de Incorporação de Tecnologias no SUS (CONITEC). Diretriz Nacional de Assistência ao Parto Normal: protocolo, relatório de recomendação [Internet]. Brasília: Ministério da Saúde; 2016 [citado 2024 Ago 16]. Disponível em: https://portaldeboaspraticas.iff.fiocruz.br/wp-content/uploads/2018/09/Relatorio_Diretriz-PartoNormal_CP.pdf
16. Benfield RD. Hydrotherapy in labor. J Nurs Scholarsh. 2002;34(4):347-52. doi:10.1111/j.1547-5069.2002.00347.x.
17. Mackey MM. Use of water in labor and birth. Clin Obstet Gynecol. 2001 Dec;44(4):733-49. doi: 10.1097/00003081-200112000-00011
18. Weaver MH. Water birth in the hospital setting. Nurs Womens Health. 2014 Oct;18(5):365-9. doi:10.1111/1751-486X.12144
19. Odent M. Água e sexualidade: a importância do parto ecológico. [S.l.]: [s.n.]; 1991. 153 p.
20. Lessa HF, Tyrrell MAR, Alves VH, Rodrigues DP. Choosing the home planned childbirth: a natural and drug free option. Rev Pesqui Cuid Fundam (Online). 2018 Oct;10(4):1118-22. doi:10.9789/2175-5361.2018.v10i4.1118-1122
21. Mendes KDS, Silveira RCPC, Galvão CM. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto Contexto Enferm. 2008 Out-Dez;17(4):758-64. doi:10.1590/S0104-07072008000400018
22. Botelho LLR, Cunha CCA, Macedo M. O método da revisão integrativa nos estudos organizacionais. Gest Soc. 2011;5(11):121-36. doi:10.21171/ges.v5i11.1220
23. Peters MDJ, Godfrey CM, McInerney P, Soares CB, Khalil H, Parker D. The Joanna Briggs Institute reviewers' manual 2015: methodology for JBI scoping reviews [Internet]. Adelaide: JBI; 2015 [citado 2022 Out 16]. Disponível em: http://joannabriggs.org/assets/docs/sumari/Reviewers-Manual_Methodology-for-JBI.Scoping-Reviews_2015_v2.pdf
24. Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018 Oct 2;169(7):467-73. doi:10.7326/M18-0850
25. Brasil. Lei nº 9.610, de 19 de fevereiro de 1998. Altera, atualiza e consolida a legislação sobre direitos autorais e dá outras providências. Lex: Coletânea de Legislação e Jurisprudência. 1998 fev 19;62:1-7.
26. Lim KMX, Tong PSY, Chong YS. A comparative study between the pioneer cohort of waterbirths and conventional vaginal deliveries in an obstetrician-led unit in Singapore. Taiwan J Obstet Gynecol. 2016 Jun;55(3):363-7. doi:10.1016/j.tjog.2016.03.003
27. Kavosi Z, Keshtkaran A, Setoodehzadeh F, Kasraeian M, Khammarnia M, Eslahi M. A comparison of mothers' quality of life after normal vaginal, cesarean, and water birth deliveries. Int J Community Based Nurs Midwifery. 2015 Jul;3(3):198-204. PMID: 26171408; PMCID: PMC4495327. Disponível em: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4495327/
28. Cooper M, McCutcheon H, Warland J. A critical analysis of Australian policies and guidelines for water immersion during labour and birth. Women Birth. 2017 Oct;30(5):431-41. doi:10.1016/j.wombi.2017.04.001
29. Seed E, Kearney L, Weaver E, Ryan EG, Nugent R. A prospective cohort study comparing neonatal outcomes of waterbirth and land birth in an Australian tertiary maternity unit. Aust N Z J Obstet Gynaecol. 2023 Feb;63(1):59-65. doi:10.1111/ajo.13555
30. Menakaya U, Albayati S, Vella E, Fenwick J, Angstetra D. A retrospective comparison of water birth and conventional vaginal birth among women deemed to be low risk in a secondary level hospital in Australia. Women Birth. 2013 Jun;26(2):114-8. doi:10.1016/j.wombi.2012.06.003
31. Harper B. Birth, bath, and beyond: the science and safety of water immersion during labor and birth. J Perinat Educ. 2014;23(3):124-34. doi:10.1891/1058-1243.23.3.124
32. Burns EE, Hunter L, Rodd Z, MacLeod M, Smith L. Developing and evaluating an online learning tool to improve midwives’ accuracy of visual estimation of blood loss during waterbirth: an experimental study. Midwifery. 2019 Jan;68:65-73. doi:10.1016/j.midw.2018.10.004
33. Maude RM, Kim M. Getting into the water: a prospective observational study of water immersion for labour and birth at a New Zealand District Health Board. BMC Pregnancy Childbirth. 2020 May;20(1):312. doi:10.1186/s12884-020-03007-6
34. Henderson J, Burns E, Regalia AL, Casarico G, Boulton MG, Smith L. Labouring women who used a birthing pool in obstetric units in Italy: prospective observational study. BMC Pregnancy Childbirth. 2014 Jan;14:17. doi:10.1186/1471-2393-14-17
35. Ulfsdottir H, Saltvedt S, Edqvist M, Georgsson S. Management of the active second stage of labor in waterbirths compared with conventional births: a prospective cohort study. Midwifery. 2022 Apr;107:103283. doi:10.1016/j.midw.2022.103283.
36. Uccella S, Manzoni P, Militello MA, Bosco M, Porcari I, Lanzo G, et al. Neonatal outcomes of water delivery versus land delivery: a retrospective propensity score weighted study. Am J Perinatol. 2023 May;40(10):1140-6. doi:10.1055/s-0043-1768961.
37. Lewis L, Hauck YL, Butt J, Hornbuckle J. Obstetric and neonatal outcomes for women intending to use immersion in water for labour and birth in Western Australia (2015–2016): a retrospective audit of clinical outcomes. Aust N Z J Obstet Gynaecol. 2018 Oct;58(5):539-47. doi:10.1111/ajo.12758
38. Bashaikh S, Mahboub F, Orabi A. Perception and knowledge of Saudi women about water birth: a cross-sectional study. Belitung Nurs J. 2022;8(5):422-30. doi:10.33546/bnj.2185
39. Camargo JCS, Varela V, Ferreira FM, Chofakian CBN, Osava RH, Araújo NM, et al. Perineal outcomes and its associated variables of water births versus non-water births: a cross-sectional study. Rev Bras Saude Matern Infant. 2019;19(4):777-86. doi:10.1590/1806-93042019000400003
40. Yorgancı A, Buyuk GN, Akyol M, Gündüz Ö, Seven B, Engin-Ustun Y. The effects of water immersion during first stage of labor on postpartum systemic inflammatory response. Z Geburtshilfe Neonatol. 2021;225(3):251-6. doi:10.1055/a-1370-0620
41. Sert UY, Ozel S, Neselioglu S, Erel O, Ustun YE. Water immersion during labour and effects on oxidative stress. Fetal Pediatr Pathol. 2020;39(3):185-93. doi:10.1080/15513815.2019.1651801
42. Nutter E, Shaw-Battista J, Marowitz A. Waterbirth fundamentals for clinicians. J Midwifery Womens Health. 2014 May;59(3):350-4. doi:10.1111/jmwh.12193
43. Enning C. Aqua-midwifery & Aqua-obstetrics. Stuttgart: Sonntag Verlag; 2003.
44. Cluett ER, Burns E. Immersion in water in labour and birth. Cochrane Database Syst Rev. 2014;(2):CD000111. doi:10.1002/14651858.CD000111.pub3
45. The American College of Nurse-Midwives. Hydrotherapy during labor and birth: position statement [Internet]. Silver Spring (MD): ACNM; 2014 Apr [citado 2022 Set 17]. Disponível em: https://www.midwife.org/acnm/files/ACNMLibraryData/UPLOADFILENAME/000000000286/Hydrotherapy-During-Labor-and-Birth-April-2014.pdf
46. Women and Newborn Health Service. Labour and/or birth using water. King Edward Memorial Hospital. Government of Western Australia, North Metropolitan Health Service, Women and Newborn Health Service; 2009 [revised 2016 Oct; citado 2022 Set 17]. Disponível em: https://www.wnhs.health.wa.gov.au
47. Zanetti-Dällenbach RA, Tschudin S, Zhong XZ, Holzgreve W, Lapaire O, Hösli I. Maternal and neonatal infections and obstetrical outcome in water birth. Eur J Obstet Gynecol Reprod Biol. 2007 Jan;134(1):37-43. doi:10.1016/j.ejogrb.2006.09.012
48. Paterson-Brown S, Howell C, eds. Managing obstetric emergencies and trauma: the MOET course manual. 3rd ed. Cambridge: Cambridge University Press; 2014. doi:10.1017/CBO9781316666043
49. Ross-Davie M, Brodrick A, Randall W, et al. Labour and birth. Best Pract Res Clin Obstet Gynaecol. 2021 Oct;76:3-17. doi:10.1016/j.bpobgyn.2021.03.011
Funding and Acknowledgments:
There is no external funding for this research. The costs are borne by the authors.
Data Availability Statement
No databases were generated in this study. The information presented is described in the body of the article.
Conflict of Interest Statement
Nothing to declare.
Authorship Criteria (Author Contributions)
Author 1 – Isabelle Souza Chies. Contributions: Data collection; Methodology; Formal analysis; Draft writing.
Author 2 – Júnia Aparecida Laia da Mata Contributions: Research project management; Research project guidance; Methodology; Data curation; Formal analysis; Writing – revision and editing.
Author 3 – Clara Fróes de Oliveira Sanfelice. Contributions: Data curation; Writing – manuscript revision.
Author 4 – Gabriela Pagano. Contributions: Data curation; Drafting.
Scientific Editor: Ítalo Arão Pereira Ribeiro. Orcid: https://orcid.org/0000-0003-0778-1447
Rev Enferm Atual In Derme 2026;100(2): e026052
![]()