ARTICLE TYPE: INTEGRATIVE LITERATURE REVIEW
DESAFIOS MULTIFATORIAIS NO MANEJO DA DOR ONCOLÓGICA PELA ENFERMAGEM: UMA REVISÃO INTEGRATIVA
MULTIFACTORIAL CHALLENGES IN NURSING MANAGEMENT OF ONCOLOGIC PAIN: AN INTEGRATIVE REVIEW
DESAFÍOS MULTIFACTORIALES EN EL MANEJO DEL DOLOR ONCOLÓGICO POR PARTE DE LA ENFERMERÍA: UNA REVISIÓN INTEGRADORA
https://doi.org/10.31011/reaid-2026-v.100-n.2-art.2741
1 Renata da Silva Lopes
2 Giovani Basso da Silva
3 Paloma Rodrigues Spies
4 João Gabriel Toledo de Medeiros
5 Eliane Goldberg Rabin
Registered Nurse. Master's Student in the Graduate Program in Nursing, Federal University of Health Sciences of Porto Alegre (UFCSPA). Porto Alegre, RS, Brazil. Email: enf.renatalopes@gmail.com. ORCID: 0000-0001-6423-9414.
2Registered Nurse. Master's Student in the Graduate Program in Pediatrics, Federal University of Health Sciences of Porto Alegre (UFCSPA). Porto Alegre, RS, Brazil. Email: gbasso70@gmail.com. ORCID: 0000-0002-3108-445X
3Undergraduate Nursing Student, Federal University of Health Sciences of Porto Alegre (UFCSPA). Porto Alegre, RS, Brazil. Email palomarodrigues.1996@hotmail.com.com. ORCID: 0009-0006-8005-3939
4Registered Nurse. Doctoral Student in the Graduate Program in Pediatrics, Child and Adolescent Health, Federal University of Health Sciences of Porto Alegre (UFCSPA). Porto Alegre, RS, Brazil. Email: joaogt@ufcspa.edu.br. ORCID: 0000-0002-2789-9189.
5Registered Nurse. PhD in Medical Sciences, Federal University of Rio Grande do Sul (UFRGS). Associate Professor in the Undergraduate Nursing Program and the Professional Master's Program in Nursing, Federal University of Health Sciences of Porto Alegre (UFCSPA). Porto Alegre, RS, Brazil. Email: elianer@ufcspa.edu.br. ORCID: 0000-0003-1496-0523
Corresponding Author
Renata da Silva Lopes
8450 Senador Salgado Avenue, Viamão, RS, Brazil, ZIP Code 94440-000. Phone: +55 (51) 99706-8604. Email: enf.renatalopes@gmail.com
Submission: 02-03-2026
Approval: 11-05-2026
ABSTRACT
Introduction: Oncologic pain is a prevalent, complex, and multidimensional symptom that affects a substantial proportion of patients with cancer, particularly in advanced stages of the disease. Effective pain management is fundamental to preserving quality of life, and nurses play a pivotal role in this domain of care. Nevertheless, a range of interrelated factors compromises the delivery of optimal pain management, contributing to persistent undertreatment and preventable suffering. Objective: To examine the challenges encountered by nursing professionals in the management of pain among patients with cancer, considering the multiple factors that impact this clinical practice. Method: An integrative literature review was conducted through a systematic search of national and international databases covering the period from 2014 to 2024. Full-text articles published in Portuguese, English, and Spanish that explicitly addressed barriers experienced by nursing professionals in the management of oncologic pain were considered. A total of 14 studies met the inclusion criteria and comprised the final sample, and these were analyzed using descriptive and thematic approaches. Results: The findings identified multifactorial challenges, organized into six principal categories: deficiencies in technical and pharmacological knowledge; misconceptions and negative attitudes toward opioid use; organizational and structural barriers; weaknesses in pain assessment, communication, and documentation; gaps in professional training and support; and limited integration of psychosocial and spiritual dimensions of care. Collectively, these factors contribute to delays in the initiation of analgesia and to the persistent undertreatment of pain. Conclusion: Management of oncological pain by the nursing team remains a complex and multifaceted challenge, shaped by individual, institutional, and educational factors. Investment in continuing education, clinical protocols, organizational support, and comprehensive care is essential to enhance nursing practice and reduce suffering among patients with cancer.
Keywords: Pain Management; Neoplasms; Nursing Care; Barriers to Health Care.
RESUMO
Introdução: A dor oncológica é um sintoma frequente, complexo e multidimensional, presente em grande parte dos pacientes com câncer, especialmente nos estágios avançados da doença. Seu manejo adequado é essencial para a qualidade de vida, e a enfermagem ocupa posição central nesse cuidado. Contudo, diversos fatores dificultam uma assistência efetiva, resultando em subtratamento e sofrimento evitável. Objetivo: Analisar as dificuldades enfrentadas pela equipe de enfermagem no manejo da dor em pacientes com câncer, considerando os múltiplos fatores que impactam essa prática assistencial. Método: Trata-se de uma revisão integrativa da literatura, com busca realizada em bases nacionais e internacionais entre 2014 e 2024. Foram incluídos artigos completos, nos idiomas português, inglês e espanhol, que abordassem diretamente barreiras vivenciadas pela enfermagem no manejo da dor oncológica. Ao final, 14 estudos compuseram a amostra, sendo analisados de forma descritiva e temática. Resultados: Os estudos revelaram dificuldades multifatoriais, agrupadas em seis categorias: déficit de conhecimento técnico e farmacológico; crenças e atitudes equivocadas sobre o uso de opioides; barreiras organizacionais e estruturais; fragilidades na avaliação, comunicação e documentação da dor; lacunas na formação e no suporte profissional; e limitada abordagem das dimensões psicossociais e espirituais. Tais fatores contribuem para atrasos na analgesia e para o subtratamento da dor. Conclusão: O manejo da dor oncológica pela enfermagem permanece um desafio complexo, influenciado por aspectos individuais, institucionais e formativos. Investir em educação continuada, protocolos assistenciais, suporte organizacional e cuidado integral é fundamental para qualificar a prática e reduzir o sofrimento do paciente oncológico.
Palavras-chave: Manejo da Dor; Neoplasias; Cuidados de Enfermagem; Barreiras à Assistência à Saúde.
RESUMEN
Introducción: El dolor oncológico constituye un síntoma frecuente, complejo y multidimensional, presente en una proporción significativa de pacientes con cáncer, especialmente en los estadios avanzados de la enfermedad. Su adecuado manejo resulta fundamental para preservar la calidad de vida, siendo la enfermería un pilar esencial en este ámbito asistencial. No obstante, múltiples factores dificultan una atención efectiva, lo que se traduce en tratamiento insuficiente y sufrimiento evitable. Objetivo: Analizar las dificultades a las que se enfrenta el equipo de enfermería en el manejo del dolor en pacientes oncológicos, considerando los diversos factores que condicionan esta práctica asistencial. Método: Se trata de una revisión integradora de la literatura, con búsqueda realizada en bases de datos nacionales e internacionales entre 2014 y 2024. Se incluyeron artículos a texto completo, publicados en portugués, inglés y español, que abordaran de forma directa las barreras experimentadas por la enfermería en el manejo del dolor oncológico. Finalmente, la muestra quedó constituida por 14 estudios, que fueron analizados desde una perspectiva descriptiva y temática. Resultados: Los estudios identificaron dificultades de carácter multifactorial, organizadas en seis categorías: déficit de conocimiento técnico y farmacológico; creencias y actitudes erróneas sobre el uso de opioides; barreras organizativas y estructurales; debilidades en la valoración, comunicación y registro del dolor; carencias en la formación y en el apoyo profesional; y limitada consideración de las dimensiones psicosociales y espirituales. Estos factores contribuyen a retrasos en la administración de la analgesia y al tratamiento insuficiente del dolor. Conclusión: El manejo del dolor oncológico por parte de la enfermería continúa representando un desafío complejo, condicionado por factores individuales, institucionales y formativos. Invertir en formación continuada, protocolos asistenciales, apoyo organizativo y atención integral resulta fundamental para cualificar la práctica y reducir el sufrimiento del paciente oncológico.
Palabras clave: Manejo del Dolor; Neoplasias; Cuidados de Enfermería; Barreras para la Atención Sanitaria.
INTRODUCTION
Pain is among the most prevalent and debilitating symptoms experienced by individuals with cancer, occurring across all stages of the disease continuum, from initial diagnosis to advanced disease progression(1). As a multidimensional phenomenon, pain extends beyond physical manifestations to encompass emotional, social, and spiritual dimensions, thereby exerting a substantial impact on the quality of life of individuals living with malignant neoplasms(2). In adults, cancer-related pain may be classified as acute or chronic. Acute pain is typically characterized by a sudden onset and is commonly associated with diagnostic procedures, cancer treatments, or tumor progression, generally presenting as a short-term condition. Chronic pain, by contrast, persists or recurs for longer than three months and may arise from the malignancy itself, metastatic spread, or treatment-related interventions(3).
The literature indicates that approximately 50% of individuals undergoing active cancer treatment and up to 90% of those with terminal-stage disease experience pain(4). These findings highlight the critical importance of effective and compassionate pain management as a fundamental component of comprehensive oncology care.
Within this context, the nursing team plays a pivotal role in cancer pain management, as it is responsible for a substantial proportion of the direct and continuous care provided to patients across different healthcare settings. Nurses are the healthcare professionals who interact most frequently with patients during hospitalization and in outpatient care, placing them in a strategic position to assess pain promptly, implement analgesic interventions, and monitor patients’ responses to prescribed therapies(5).
Clinical guidelines emphasize that comprehensive pain assessment is a cornerstone of effective pain management, as incomplete or inadequate evaluations are frequently associated with suboptimal pain control. Accordingly, all individuals with cancer should undergo systematic and ongoing pain assessments, including the identification of the underlying causes of pain and the determination of the most appropriate therapeutic approaches. Such assessments support informed, safe, and effective clinical decision-making(3).
Despite the importance of this role, cancer pain management remains a complex challenge for nursing professionals and is shaped by multiple factors that may hinder the delivery of safe and effective care. Evidence suggests that the difficulties nurses encounter in managing pain among individuals with cancer are associated with several dimensions, including gaps in technical and scientific knowledge related to pain assessment and pharmacological management, concerns regarding opioid administration, the absence of institutional protocols, ineffective communication within the multidisciplinary team, and subjective factors such as personal beliefs, previous experiences, and attitudes toward pain(6–7). These barriers can compromise the quality and comprehensiveness of care, contributing to inadequate pain management, preventable suffering, and dissatisfaction among patients and their families, including those receiving oncology palliative care(8).
Given the significance and complexity of caring for patients with cancer who experience pain, this integrative review aims to analyze the challenges faced by the nursing team in the management of cancer-related pain, considering the multiple factors that influence this aspect of clinical practice.
METHODOLOGY
This study consists of an integrative literature review, a methodological approach that enables the comprehensive and systematic identification, analysis, and synthesis of the available scientific evidence on a given topic. The review was conducted in accordance with the stages proposed by Souza, Silva, and Carvalho(9), which include the formulation of the research question, establishment of eligibility criteria, development of the search strategy, selection and categorization of studies, data extraction and analysis, and presentation of the findings.
The guiding research question was developed using the PICo framework to enhance the sensitivity of the search strategy. Within this framework, the population consisted of individuals with cancer, the phenomenon of interest was pain management, and the context encompassed the challenges experienced by the nursing team. Based on these elements, the following research question was formulated: “What challenges are faced by the nursing team in the management of pain among patients with cancer?”
Studies were considered eligible if they were available in full text, presented a clearly described methodology, were published between 2014 and 2024, and were written in Portuguese, English, or Spanish, provided that they directly addressed the challenges faced by the nursing team in the management of cancer-related pain. The selected time frame encompassed the most recent decade of publications, ensuring that the evidence reflected contemporary practices and evolving care guidelines. Editorials, letters to the editor, conference abstracts, duplicate publications, and studies that did not address the research question were excluded from the sample. Studies involving pediatric populations or focusing on other healthcare professionals were also excluded to preserve the focus on the nursing context within adult oncology care.
The search strategy was developed using descriptors from the Health Sciences Descriptors (DeCS) and terms from the Medical Subject Headings (MeSH), combined with the Boolean operators AND and OR, as presented in Table 1. The search strings were adapted to the indexing characteristics and search requirements of each database, and the complete search syntaxes are presented in Table 2.
Table 1 - Search descriptors.
|
Key Concept |
Portuguese (DeCS) |
English (MeSH) |
Synonyms / Alternative Terms |
|
Pain |
Dor |
Pain |
Pain relief, pain control, painful symptom |
|
Neoplasms |
Neoplasias |
Neoplasms |
Cancer, tumor, oncologic disease |
|
Nursing |
Equipe de Enfermagem / Cuidados de Enfermagem |
Nursing Staff / Nursing Care |
Nursing professionals, nursing practice |
|
Pain Management |
Manejo da Dor |
Pain Management |
Pain control, pain treatment, pain management strategies |
|
Healthcare Barriers |
Barreiras à Assistência à Saúde |
Health Care Barriers |
Obstacles, limitations in care |
|
Professional Attitudes |
Atitude do Pessoal de Saúde |
Health Personnel Attitudes |
Team attitudes, professional perceptions |
Source: Prepared by the authors.
Table 2 - Search strategies used in the databases.
|
DATABASE |
SEARCH STRATEGY |
|
PubMed (MeSH Terms) |
("Pain Management"[MeSH Terms] OR "Pain"[MeSH Terms]) AND ("Neoplasms"[MeSH Terms]) AND ("Nursing"[MeSH Terms] OR "Nursing Staff"[MeSH Terms]) AND ("Health Care Barriers"[MeSH Terms] OR "Attitude of Health Personnel"[MeSH Terms]) |
|
Scopus (TITLE-ABS-KEY fields)
|
TITLE-ABS-KEY("pain management" OR "pain") AND TITLE-ABS-KEY("neoplasms" OR "cancer") AND TITLE-ABS-KEY("nursing" OR "nursing staff") AND TITLE-ABS-KEY("barriers" OR "difficulties" OR "attitude of health personnel") |
|
SciELO (simple search using Boolean operators) |
("manejo da dor" OR "dor") AND ("câncer" OR "neoplasias") AND ("enfermagem" OR "equipe de enfermagem") AND ("barreiras" OR "dificuldades" OR "atitudes dos profissionais de saúde") |
|
BVS (Virtual Health Library – advanced search using DeCS)
|
tw:("manejo da dor" OR "controle da dor" OR "dor") AND tw:("neoplasias" OR "câncer") AND tw:("enfermagem" OR "equipe de enfermagem") AND tw:("barreiras à assistência" OR "dificuldades" OR "atitude do pessoal de saúde") |
|
Web of Science – Search Strategy (English) |
TS=("pain management" OR "pain") AND TS=("neoplasms" OR "cancer") AND TS=("nursing" OR "nursing staff") AND TS=("barriers" OR "difficulties" OR "attitude of health personnel") |
Source: Prepared by the authors.
Data collection was conducted in May 2025. All retrieved records were imported into the Rayyan® platform(10), which was used to support the study screening process. This platform enables semi-automated study selection, organization of screening decisions, and collaboration among reviewers, thereby enhancing the transparency, traceability, and efficiency of the screening process.
The screening process was conducted in two phases. First, titles and abstracts were reviewed to identify potentially eligible studies. The selected articles were cataloged in a Microsoft Excel spreadsheet containing information on authorship, journal, study objectives, country of origin, principal findings, and a preliminary relevance assessment. Subsequently, full-text articles were reviewed and documented in a second spreadsheet, which included detailed information on study design, sample characteristics, study setting, and key findings.
The study selection process was organized according to a flow diagram adapted from the PRISMA 2020 Statement(11), as presented in Figure 1.
Figure 1 - PRISMA 2020 flow diagram of the study selection process.
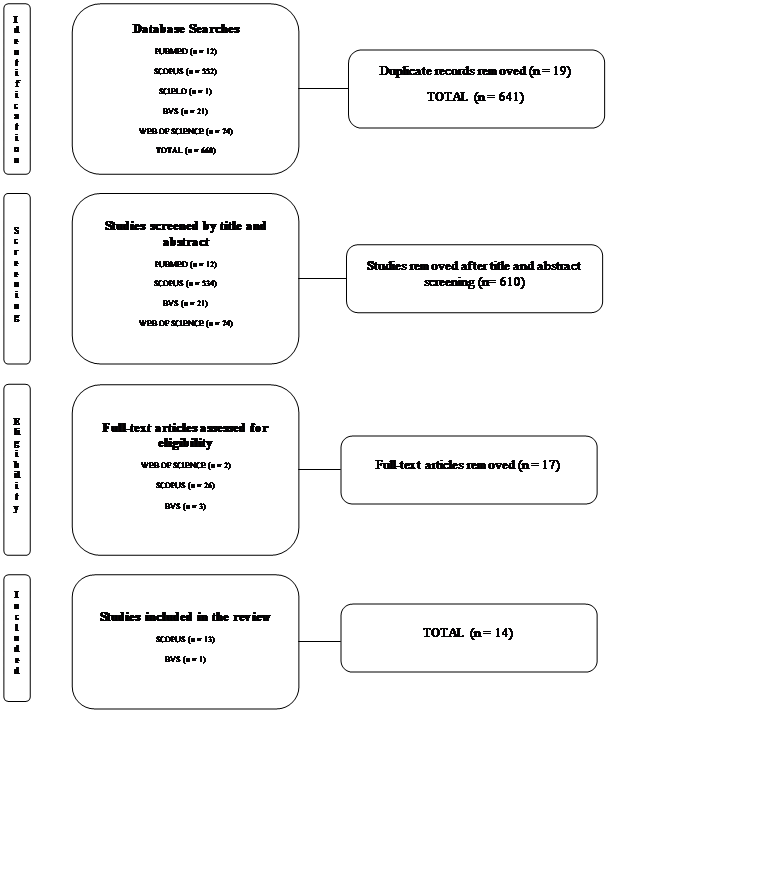
Source: Prepared by the authors.
Figure 1 illustrates the study selection process adopted in this review through a flow diagram adapted from the PRISMA 2020 Statement (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)(11).
Data were analyzed using a descriptive and thematic approach(9), supported by the development of a synoptic table summarizing the main characteristics of the included studies. The quality of evidence was assessed using the GRADE system(12), considering the domains of risk of bias, consistency, precision, indirectness of evidence, and publication bias. Subsequently, the findings were organized into thematic categories based on similarities in the challenges reported by the nursing team regarding cancer pain management. This approach enabled the identification of patterns, inconsistencies, and knowledge gaps, thereby supporting a critical interpretation of the findings in light of the existing scientific literature.
RESULTS
The database search identified 14 articles that met the eligibility criteria and were included in this integrative review. These studies were published between 2015 and 2024 and were fully aligned with the predefined inclusion criteria. Most publications were concentrated between 2019 and 2024, suggesting growing scientific interest in the topic. The studies were conducted in a variety of countries, with a predominance of research originating from Asia and the Middle East, particularly China, Iran, and Jordan. Additional contributions were identified from Europe (Norway), Oceania (Australia), Africa (Kenya), and Latin America (Brazil). This geographical distribution underscores the global relevance of the topic while also reflecting the challenges associated with cancer pain management across different low- and middle-income settings.
The Knowledge and Attitudes Survey Regarding Pain (KASRP) was the most frequently applied instrument, appearing in several studies. Quantitative research employing cross-sectional designs predominated, although qualitative investigations and integrative reviews were also identified, particularly those addressing organizational and systemic barriers to effective cancer pain management.
The GRADE assessment indicated a low overall level of evidence across the included studies, primarily due to the predominance of observational and cross-sectional designs. Despite this limitation, the findings demonstrated consistency across different countries and healthcare settings.
Table 3 - Summary of studies included in the integrative review.
|
Reference (Author, Year, Country) |
Design / Sample |
Instrument |
Main Findings (Focus on Challenges) |
Conclusions / Recommendations |
GRADE Level of Evidence |
|
Yu et al., 2021 (China)(13) |
Cross-sectional, 505 nurses |
KASRP |
Knowledge deficits (mean score 56%) and misconceptions regarding opioids |
Continuous training programs and correction of misconceptions |
Low |
|
Li et al., 2021 (China)(14) |
Cross-sectional, 982 nurses |
KASRP |
Insufficient knowledge regarding opioid titration and administration |
Continuing education using active-learning strategies and support for less experienced nurses |
Low |
|
Ferreira et al., 2019 (Brazil)(15) |
Cross-sectional, 126 nurses |
Ramos (1994) |
Inadequate knowledge (45.9%) and dysfunctional beliefs regarding opioids |
Continuing education and reflection on analgesic practices |
Low |
|
Utne et al., 2019 (Norway)(16) |
Cross-sectional, 312 nurses |
NKASRP |
Pharmacological knowledge deficits and subjectivity in pain assessment |
Clinical training with cultural sensitivity and emphasis on pharmacology |
Moderate |
|
Sadeghy et al., 2016 (Iran)(17) |
Descriptive, 49 nurses |
BQ-II |
Negative attitudes and beliefs concerning addiction and severe adverse effects |
Educational interventions to correct misconceptions |
Low |
|
Onsongo, 2020 (Kenya)(18) |
Qualitative, 25 nurses |
Interviews and observation |
Lack of protocols, excessive workload, and fear of opioid use |
Institutional protocols and strengthening of multidisciplinary care |
Low |
|
Mangolian Shahrbabaki et al., 2024 (Iran)(19) |
Qualitative, 24 nurses |
Open-ended interviews |
Failures in care processes, inadequate infrastructure, and patient resistance |
Health education and structural improvements |
Low |
|
Toba et al., 2019 (Palestine)(20) |
Cross-sectional, 220 nurses |
Adapted questionnaire |
Inadequate pain assessment and restrictions on opioid use |
Training and improved communication with physicians |
Low |
|
Othman et al., 2022 (Jordan)(21) |
Cross-sectional, 502 nurses |
Questionnaire based on Toba et al. (2019) |
Restrictive regulations and gaps in interprofessional communication |
Policy review and improved nurse–physician coordination |
Moderate |
|
Phillips et al., 2015 (Australia)(22) |
Mixed-methods cross-sectional, 62 nurses |
Online questionnaire |
Lack of coordination among providers and absence of specific guidelines |
National guidelines and structured clinical pathways |
Low |
|
Bartoszczyk & Gilbertson-White, 2015 (USA)(23) |
Literature review, 9 studies |
Several validated instruments |
Effective interventions for improving knowledge, with limited impact on attitudes |
Presence of specialists and ongoing programs to enhance sustainability |
Moderate |
|
Oliveira et al., 2016 (Brazil)(24) |
Narrative review, 14 articles |
Integrative review |
Opioid phobia, educational gaps, and underuse of non-pharmacological approaches |
Investment in education and continuing professional development |
Low |
|
Bouya et al., 2019 (Iran)(25) |
Systematic review, 12 studies |
KASRP and others |
Knowledge deficits and negative attitudes |
Structured programs and interdisciplinary approaches |
High |
|
Alsaiari et al., 2024 (Saudi Arabia)(26) |
Scoping review, 20 studies |
KASRP and interviews |
Underdosing and inadequate pain documentation |
Comprehensive programs and expanded educational initiatives |
High
|
Source: Prepared by the authors.
The thematic analysis of the included studies resulted in the identification of six categories that reflect the principal challenges faced by nurses in cancer pain management: deficiencies in technical and pharmacological knowledge; misconceptions and negative attitudes toward opioid use; organizational and structural barriers; weaknesses in pain assessment, communication, and documentation; gaps in training, support, and professional experience; and the psychosocial and spiritual dimensions of care.
Table 4 - Summary of thematic categories and key findings from the analyzed studies.
|
CATEGORY |
STUDIES (AUTHOR, YEAR) |
MAIN FINDINGS AND REPORTED CHALLENGES |
INTERPRETIVE SYNTHESIS AND IMPLICATIONS |
|
1. Deficiencies in Technical and Pharmacological Knowledge |
Yu (2020); Li (2021); Bouya (2018); Othman (2022); Utne (2018); Alsaiari (2024); Bartoszczyk & Gilbertson-White (2015) |
Knowledge scores below 60% on KASRP assessments, particularly in areas related to opioid pharmacology, dose titration, rescue dosing, and adverse effects. Overestimation of the risk of respiratory depression, misconceptions regarding physical dependence, inconsistent use of pain assessment scales, and limited knowledge of multimodal pain management strategies. |
Insufficient knowledge compromises effective pain management and contributes to undertreatment. Continuous professional development and the integration of pain physiology, pharmacology, and non-pharmacological management strategies into healthcare education are essential, with an emphasis on clinical cases and decision-making skills. |
|
2. Misconceptions and Negative Attitudes Toward Opioid Use |
Sadeghy (2016); Yu (2020); Li (2021); Ferreira (2019); Utne (2018); Mangolian Shahrbabaki (2024); Othman (2022) |
Misconceptions that patients inevitably develop dependence or addiction, that cancer-related pain is unavoidable, and that opioid-related adverse effects cannot be adequately managed. Reported concerns included sedation, nausea, and cognitive impairment. Some nurses endorsed the use of placebos or delayed analgesic administration until physician authorization was obtained. |
Attitudinal barriers reflect persistent stigma and institutional fears. Educational interventions should incorporate ethical and attitudinal dimensions, fostering critical reflection on prevailing beliefs and evidence-based opioid use. Healthcare institutions should invest in structured continuing education programs. |
|
3. Organizational and Structural Barriers |
Onsongo (2020); Toba (2019); Phillips (2015); Mangolian Shahrbabaki (2024); Othman (2022); |
Excessive workload, staffing shortages, and the absence of institutional protocols and accessible guidelines. Additional barriers included restrictive opioid regulations, ineffective interprofessional communication, and delays in analgesic administration (reported in up to 56.4% of cases) resulting from the need for physician authorization. Limited access to non-pharmacological interventions and logistical constraints were also identified. |
Organizational conditions undermine effective pain control. The implementation of clinical pathways, adequate staffing levels, and greater nursing autonomy within pain-management protocols are necessary. |
|
4. Weaknesses in Pain Assessment, Communication, and Documentation |
Toba (2019); Phillips (2015); Oliveira (2016); Onsongo (2020); Bartoszczyk & Gilbertson-White (2015) |
Deficiencies in active listening, incomplete documentation, ineffective communication among healthcare professionals and with patients, and the undervaluation of patients’ subjective reports of pain. Other challenges included inconsistencies between pain assessment and reassessment, as well as insecurity among professionals regarding the use of pain assessment scales. |
Communication deficits contribute to the undertreatment of pain and may prolong patient suffering. The implementation of standardized pain assessment protocols, documentation audits, and interdisciplinary rounds may enhance the continuity of care. |
|
5. Gaps in Training, Support, and Professional Experience |
Li (2021); Ferreira (2019); Bouya (2018); Bartoszczyk & Gilbertson-White (2015); Alsaiari (2024); |
More experienced nurses tended to achieve better outcomes; however, insufficient specialized training and the lack of continuing education programs contributed to the persistence of unsafe practices. Although isolated educational interventions were associated with improvements in knowledge, their effects on attitudes were limited in the absence of institutional support. The authors also pointed to the lack of pain specialists available to provide clinical mentorship. |
Initial professional education alone is insufficient to support competent pain management practices. Ongoing learning pathways and specialized mentorship programs should be implemented, integrating technical, humanistic, and non-pharmacological components. |
|
6. Psychosocial and Spiritual Dimensions of Care |
Oliveira (2016); Mangolian Shahrbabaki (2024); Ferreira (2019) |
Limited recognition of the concept of total pain and of the influence of emotional and spiritual factors on cancer-related suffering. Non-pharmacological interventions, including massage, comfort measures, and spiritual support, were underutilized. |
Pain should be recognized as a multidimensional experience. Accordingly, nursing care should incorporate psychosocial and non-pharmacological interventions into the care plan to promote symptom relief and strengthen the therapeutic relationship. |
Source: Prepared by the authors.
Overall, the findings suggest that the challenges faced by the nursing team in the management of cancer-related pain are multifactorial, encompassing knowledge deficits, attitudinal barriers, structural constraints, and insufficient organizational support.
DISCUSSION
The findings of this study provide the foundation for the critical discussion presented in this section, which aims to integrate the results with the existing literature and examine their implications for clinical practice and nursing education. The identified categories are discussed in the form of thematic subsections.
1. DEFICIENCIES IN TECHNICAL AND PHARMACOLOGICAL KNOWLEDGE
The findings revealed that deficiencies in technical and pharmacological knowledge substantially compromise the management of cancer-related pain. The studies included in this review identified uncertainties regarding opioid titration, difficulties in identifying adverse effects, and inconsistencies in the use of pain assessment instruments(13,14,25). These knowledge deficits directly affect the accuracy of clinical decision-making and the safety of pain management interventions.
This pattern is further supported by evidence showing that more than half of the nurses assessed demonstrated insufficient knowledge of fundamental concepts in pain pharmacology, including dose adjustment, expected adverse effects, and patient monitoring criteria(27). These findings are consistent with previous research indicating limited pharmacological competence among oncology nurses, particularly with respect to the understanding of efficacy and safety parameters, as well as the core principles of multimodal analgesia(28).
Taken together, these findings suggest that deficits in technical knowledge are consistently observed across diverse healthcare settings and may adversely affect the quality of analgesia provided. Although the predominance of observational studies precludes causal inference, the consistency of the evidence indicates that deficiencies in technical and pharmacological knowledge represent a significant challenge in clinical practice and constitute a key factor in understanding the difficulties faced by the nursing team in managing cancer-related pain.
2. MISCONCEPTIONS AND NEGATIVE ATTITUDES TOWARD OPIOID USE
Misconceptions and negative attitudes regarding opioid use emerged as significant barriers to effective cancer pain management. The studies included in this review identified concerns related to addiction, misunderstandings regarding opioid tolerance and efficacy, overestimation of adverse effects such as respiratory depression, and reluctance to adjust opioid dosages. These attitudes were often reinforced by the belief that pain is an inevitable consequence of cancer, as well as by biases directed toward specific patient groups(14,16,19). Collectively, these factors contributed to delays in analgesic treatment and reinforced overly restrictive pain management practices
Within this context, misconceptions regarding the risks of addiction and sedation have been shown to hinder adherence to evidence-based recommendations for pain management (29). Furthermore, opioid dose escalation is frequently avoided, even in the presence of severe pain, owing to unfounded concerns about tolerance and adverse effects(30). Opioid phobia has also been associated with cultural influences, negative clinical experiences, and conservative institutional narratives, contributing to more restrictive analgesic practices that may be insufficiently responsive to patients’ needs(31).
Although the evidence is derived predominantly from observational studies, the consistency of findings across the literature suggests that misconceptions and negative attitudes toward opioid use represent a substantial barrier to effective pain management. These findings highlight the need for educational interventions aimed at fostering an accurate, evidence-based, and clinically informed understanding of the therapeutic use of opioid.
3. ORGANIZATIONAL AND STRUCTURAL BARRIERS
In this review, organizational and structural barriers emerged as significant obstacles to effective cancer pain management. The studies included in this review identified the absence of clear clinical protocols, excessive workload, fragmented communication among healthcare professionals, and delays between patients’ reports of pain and the administration of analgesic therapy as some of the most frequently reported challenges(18,20,22).
The broader literature further highlights the influence of organizational factors on cancer pain management. Evidence suggests that the absence of institutional guidelines, combined with regulatory restrictions surrounding opioid use, contributes to delays in analgesic administration, even when appropriate prescriptions are available(20).
In this regard, structural deficiencies within healthcare delivery processes, including insufficient time, excessive workload, and ineffective communication, may hinder the ongoing assessment and monitoring of pain(32). Similarly, recent evidence has identified additional institutional barriers, such as medication shortages, the absence of specific clinical guidelines, an insufficient number of specialized professionals, and the centralization of services, all of which may compromise the timely and effective delivery of pain management interventions(33).
Although the evidence is derived predominantly from observational studies, the consistency of findings across diverse healthcare settings suggests that organizational barriers play a substantial role in pain management. These findings underscore the need to optimize care delivery processes, strengthen clinical protocols, and foster collaborative practices to improve cancer pain management.
4. WEAKNESSES IN PAIN ASSESSMENT, COMMUNICATION, AND DOCUMENTATION
Despite advances in oncology care, pain assessment remains a vulnerable component of clinical practice. Although pain has been recognized as the fifth vital sign, its assessment and monitoring continue to be conducted inconsistently in many healthcare settings. Patients’ reports of pain are not always adequately valued, documentation is often incomplete, and interdisciplinary communication regarding pain remains limited, all of which may contribute to the undertreatment of cancer-related pain(20,22). Furthermore, healthcare professionals have reported uncertainty in interpreting pain assessment scales and translating their findings into appropriate therapeutic adjustments, resulting in the frequent omission of structured pain reassessment(18,23).
In this context, substantial challenges in pain assessment and documentation continue to persist in nursing practice despite the recognition of pain as the fifth vital sign. Within the national context, healthcare professionals have reported difficulties in the consistent use of pain assessment scales, the accurate interpretation of these instruments, and the translation of assessment findings into clear and meaningful documentation that supports continuity of care(34). Additionally, pain-related documentation is not always completed and may lack essential information, thereby weakening communication across shifts and multidisciplinary teams and compromising clinical decision-making(34). These findings are consistent with international evidence demonstrating a lack of documented pain reassessments, inconsistencies in recordkeeping, and limited integration among pain assessment, communication, and therapeutic decision-making processes(35,36).
Taken together, these findings suggest that the challenge extends beyond the selection of pain assessment instruments and involves the establishment of a care culture in which assessment, documentation, and communication are recognized as continuous and interdependent components of safe and effective cancer pain management.
5. GAPS IN TRAINING, SUPPORT, AND PROFESSIONAL EXPERIENCE
The findings demonstrate that both educational preparation and institutional support play a crucial role in shaping nurses’ confidence in pain assessment and management. Technical competence appears to develop progressively through professional experience, whereas less experienced nurses tend to report greater apprehension regarding opioid administration and the adjustment of analgesic interventions, suggesting insecurity associated with an insufficient educational foundation(14,15). However, professional experience alone does not ensure proficiency in pain management. More experienced nurses have also reported feeling inadequately supported when making analgesic decisions, highlighting persistent gaps in organizational support and continuing education opportunities(23,25,26).
The analysis of the included studies further suggests that educational gaps persist beyond undergraduate training, particularly in relation to the interpretation of pain assessment scales, the understanding of pain mechanisms, and the integration of assessment findings into therapeutic decision-making. Recent evidence indicates that many nurses recognize the need to further develop their knowledge level and skills, suggesting that although clinical experience contributes to greater familiarity with pain management, it is insufficient to overcome structural shortcomings in professional education(27). Similarly, international studies have reported that healthcare professionals widely recognize the importance of expanding specialized training in pain management and strengthening the technical and interpersonal competencies required for safe, effective, and consistent pain assessment(28).
Thus, these findings suggest that competence in pain assessment depends not only on individual clinical experience but also on the availability of robust educational curricula, ongoing professional development opportunities, and institutional environments that effectively support clinical decision-making.
6. PSYCHOSOCIAL AND SPIRITUAL DIMENSIONS OF CARE
Although pain is often conceptualized primarily as a physical symptom, the studies included in this review indicate that individuals with cancer experience pain as a multidimensional phenomenon shaped by emotional distress, personal losses, existential concerns, and issues related to spirituality and end-of-life concerns. When these dimensions are not adequately recognized by healthcare professionals, care tends to focus predominantly on pharmacological management, resulting in only partial symptom relief and a limited approach to pain management, as it fails to address the multiple factors that intensify pain and influence its subjective experience(19,24).
Recent international evidence further underscores the influence of psychosocial factors on the experience of pain among individuals with cancer. Factors such as fear, anxiety, perceived threat, family conflicts, and disruptions in interpersonal relationships have been shown to shape pain perception and intensify overall suffering(2). Oncology nurses report that interventions such as active listening, therapeutic presence, emotional support, and empathetic communication contribute to pain relief and improved well-being, reinforcing the integrated nature of care(37).
With regard to the spiritual dimension, studies indicate that patients frequently experience existential concerns related to guilt, loss of meaning, fear of death, and threats to personal identity. Evidence further suggests that addressing these concerns with sensitivity may alleviate both emotional and physical suffering(38). When adequately trained and supported by their institutions, nurses report greater confidence in identifying spiritual pain and implementing targeted interventions(39). Nevertheless, barriers remain, including insufficient training, concerns about intruding on patients’ personal beliefs, and the absence of institutional policies that formally recognize spiritual care as an integral component of pain management(39).
In this sense, these findings suggest that the integration of psychosocial and spiritual dimensions into patient care is essential for comprehensive cancer pain management, enabling clinical practice to more effectively address the complex and multidimensional needs of patients.
LIMITATIONS AND STRENGTHS
This review has certain limitations that should be acknowledged. The use of author-defined descriptors may have reduced the sensitivity of the search strategy and contributed to the omission of potentially relevant studies employing different terminology. Moreover, the predominance of observational study designs among the included articles limits the certainty of the available evidence.
Despite these limitations, the review is strengthened by the international scope of the included studies, which encompass diverse sociocultural contexts and, in several cases, robust sample sizes, thereby broadening the understanding of the phenomenon under investigation. Another important strength lies in the integration of the findings with both recent international evidence and the national literature, highlighting the consistency of the challenges faced by nursing professionals in the management of cancer-related pain across different healthcare settings and realities.
Study Contributions
This study is expected to contribute to the advancement of knowledge and to encourage further research in the field of oncology nursing. By highlighting the challenges faced by the nursing team in managing cancer-related pain, the findings underscore the pivotal role of nursing professionals in delivering comprehensive, compassionate, and evidence-based care. Furthermore, the results may inform healthcare professionals, educators, and administrators about the need to strengthen educational training, clinical practice, and institutional support systems, thereby contributing to improvements in care quality and to the reduction of suffering among individuals with cancer.
CONCLUSION
Although pain has been extensively investigated in the pursuit of a deeper understanding and more effective management strategies, this review demonstrates that the challenges associated with its assessment in oncology care remain both relevant and persistent. The analysis identified six distinct dimensions that, although closely related, represent different aspects of clinical practice and therefore require specific approaches. Recognizing these distinctions is essential, as it enables a more precise understanding of how each challenge influences nursing practice and which strategies may contribute to improving the quality of care.
The findings reinforce that improving cancer pain management requires sustained investment in professional education, institutional support, and the cultivation of a care culture that values attentive listening, accurate documentation, and comprehensive, patient-centered care. In this context, the identified barriers should not be viewed solely as obstacles but also as reflections of the complexity inherent in cancer care. Hesitation in clinical decision-making, when not supported by adequate knowledge and organizational resources, may contribute to increased patient suffering. Conversely, the early development of both theoretical and practical competencies enables nurses to translate caution into safe and effective clinical practice, thereby avoiding inappropriate interventions and preventing unnecessary suffering among patients with cancer.
REFERENCES
1 World Health Organization. Cancer pain relief: with a guide to opioid availability. 2nd ed. Geneva: WHO; 1996.
2 National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Adult Cancer Pain. J Natl Compr Canc Netw. 2025;23(7):e250032. doi:10.6004/jnccn.2025.0032.
3 Breivik H, Cherny N, Collett B, de Conno F, Filbet M, Foubert AJ, et al. Cancer-related pain: a pan-European survey of prevalence, treatment, and patient attitudes. Ann Oncol. 2009;20(8):1420-1433. doi:10.1093/annonc/mdp001.
4 Van den Beuken-van Everdingen MHJ, Hochstenbach LMJ, Joosten EAJ, Tjan-Heijnen VCG, Janssen DJA. Update on prevalence of pain in patients with cancer: systematic review and meta-analysis. J Pain Symptom Manage. 2016;51(6):1070-1090. doi:10.1016/j.jpainsymman.2015.12.340.
5 de Munter J, Dodlek N, Khmaladze A, Parreira ST, Ullgren H, de Man R, de Jong FA, Oldenmenger WH. The role of cancer nurses in cancer-related pain management in Europe. Palliat Care Soc Pract. 2023;17:26323524231216996. doi:10.1177/26323524231216996.
6 Damar HT, Bilik O, Ozdagoglu G, Ozdagoglu A, Damar M. Scientometric overview of nursing research on pain management. Rev Latino-Am Enfermagem. 2018;26:e3051. doi: 10.1590/1518-8345.2581.3051
7 Paice JA, Ferrell B. The management of cancer pain. CA Cancer J Clin. 2011;61(3):157-182. doi:10.3322/caac.20112.
8 Nascimento JCC, Campos JS, Vieira VP, Barbosa MCR. Percepção da enfermagem sobre avaliação da dor oncológica. Rev Perspect Online Biol Saúde. 2020;10(32):51-61. doi: 10.25242/8868103220201937.
9 Souza MT, Silva MD, Carvalho R. Revisão integrativa: o que é e como fazer. Einstein (São Paulo). 2010;8(1):102-106. doi:10.1590/S1679-45082010RW1134.
10 Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan: a web and mobile app for systematic reviews. Syst Rev. 2016;5:210. doi:10.1186/s13643-016-0384-4.
11 Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71.
12 Brasil. Ministério da Saúde. Secretaria de Ciência, Tecnologia e Insumos Estratégicos. Departamento de Ciência e Tecnologia. Diretrizes metodológicas: sistema GRADE, manual de graduação da qualidade da evidência e força de recomendação para tomada de decisão em saúde. Brasília (DF): Ministério da Saúde; 2014.
13 Yu H, Gao M, Wang M, Zhang S, Ma L, Huang Y, et al. Knowledge and attitudes of Chinese oncology nurses regarding cancer pain management. Pain Management Nursing. 2021;22(2):150-158. doi: 10.1007/s13187-020-01743-z.
14 Li D, Gao L, Ren LY, Zeng X, Cui EP, Zhang LJ, et al. Knowledge and attitudes regarding cancer pain management among oncology nurses in China: a cross-sectional study. J Int Med Res. 2021;49(1):300060520979448. doi:10.1177/0300060520979448.
15 Ferreira FDS, Meira KCC, Félix RS, Oliveira IRS, Pinto CMI, Silva MAS, et al. Associated factors with the knowledge of nurses of a high complexity oncology centre in Brazil on the management of cancer pain. Ecancermedicalscience. 2019;13:928. doi:10.3332/ecancer.2019.928.
16 Utne I, Miaskowski C, Bjordal K, Paul SM, Rustøen T. Pain knowledge and attitudes among nurses in cancer care in Norway. J Pain Symptom Manage. 2019;57(3):620-627. doi: 10.1007/s13187-018-1355-3.
17 Sadeghy L, Farsani DM, Zareiyan A. Nurse attitude-related barriers to effective control of cancer pain among Iranian nurses. J Pain Symptom Manage. 2016;51(5):986-992. doi: 10.7314/apjcp.2016.17.4.2141.
18 Onsongo CN. Barriers to cancer pain management among nurses working at Kenyatta National Hospital, Kenya. Int J Afr Nurs Sci. 2020;13:100251. doi: 10.1016/j.pmn.2019.08.006.
19 Mangolian Shahrbabaki P, Nouhi E, Mohammadi E, Ramezanli S, Dehghan M. Persistence of pain and suffering in cancer patients: challenges of pain management from the perspective of nurses. Front Pain Res. 2024;23(1):45. doi: 10.3389/fpain.2024.1425036.
20 Toba HA, Samara AM, Zyoud SH. Nurses’ knowledge, perceived barriers, and practices regarding cancer pain management: a cross-sectional study from Palestine. BMC Med Educ. 2019;19(1):167. doi: 10.1186/s12909-019-1613-z.
21 Othman EH, Al-Atiyyat NM. Knowledge, perceived barriers, and practices of oncology nurses regarding cancer pain management. Pain Manag Nurs. 2022;23(1):76-85. doi: 10.29333/ejgm/12337.
22 Phillips JL, Lovell M, Luckett T, Agar M, Green A, Davidson PM. Australian survey of current practice and guideline use in adult cancer pain assessment and management: the community nurse perspective. Collegian. 2014;22(1):33–41. doi: 10.1016/j.colegn.2013.11.002.
23 Bartoszczyk DA, Gilbertson-White S. Interventions to nurse-related barriers in cancer pain management. Oncol Nurs Forum. 2015;42(6):634-641. doi:10.1188/15.ONF.634-641.
24 Oliveira AB, Fernandes AFC, Silva RM. Manuseio da dor crônica em pacientes oncológicos pela equipe de enfermagem. Rev Dor. 2016;17(3):219-224. doi:10.5935/1806-0013.20160075.
25 Bouya S, Balouchi A, Maleknejad A, Koochakzai M, Abdollahimohammad A. Cancer pain management among oncology nurses: knowledge, attitude, related factors, and clinical recommendations: a systematic review. J Cancer Educ. 2019;34(4):839-846. doi: 10.1007/s13187-018-1433-6.
26 Alsaiari SA, Alkahtani A, Almalki K, Alqahtani A, Alotaibi M. Nurses’ knowledge, perceived barriers, and practices regarding cancer pain management: a scoping review. Indian J Palliat Care. 2024;30:1-9. doi: 10.25259/IJPC_232_2023.
27 Silva BU, Yoshioka EM, Salvetti MG. Conhecimento de Enfermeiros sobre o Manejo da Dor Oncológica. Rev Bras Cancerol. 2022;68(4):e072552. doi:10.32635/2176-9745.RBC.2022v68n4.2552.
28 Dong T, Li X, Zhang Y, Wang L, Chen J, Liu H, et al. Competence and training needs in cancer pain management among nurses: a cross-sectional study. Front Med (Lausanne). 2025;12:1594859. doi:10.3389/fmed.2025.1594859.
29 Bulls HW, Chu E, Goodin BR, Liebschutz JM, Wozniak A, Schenker Y, Merlin JS. Framework for opioid stigma in cancer pain. Pain. 2022;163(2):e182-e189. doi:10.1097/j.pain.0000000000002343.
30 Charalambous A, Kaite CP, Kouta C, et al. Healthcare professionals’ perceptions on the use of opioid analgesics for the treatment of cancer-related pain in Cyprus: a mixed-method study. SAGE Open Med. 2019;7:2050312119841823. doi:10.1177/2050312119841823.
31 Harsanyi H, Papp-Zipernovszky O, et al. The stigma surrounding opioid use as a barrier to cancer-pain management: an overview of experiences with fear, shame, and poorly controlled pain in the context of advanced cancer. Curr Oncol. 2023;30(6):5835-5848. doi:10.3390/curroncol30060437.
32 Carr E. Barriers to effective pain management. J Perioper Pract. 2007;17(5):200-208. doi:10.1177/175045890701700502.
33 Mulonda JK, Havenga Y, De Villiers M. Healthcare providers’ perceptions of the cancer pain management barriers at a hospital in Zambia: a qualitative study. SAGE Open Nurs. 2023;9:23779608231197008. doi:10.1177/23779608231197008.
34 Valério AF, Silva RM, et al. Dificuldades enfrentadas pela enfermagem na aplicabilidade da dor como quinto sinal vital e os mecanismos/ações adotados: revisão integrativa. BrJP. 2019;2(1):67-71. doi:10.5935/2595-0118.20190013.
35 Dalton JA, Blau W, Carlson J, Lindley C, Greer SM, Youngblood R. Documentation of pain assessment and treatment: how are we doing? Pain Manag Nurs. 2001;2(2):54-64. doi: 10.1053/jpmn.2001.23918.
36 Morris JL, Bernard F, Bérubé M, Dube JN, Houle J, Laporta D, et al. Determinants of pain assessment documentation in intensive care units. Can J Anaesth. 2021;68(8):1176-1184. doi:10.1007/s12630-021-02022-1.
37 Lyu XC, Zhang Y, Li Q, et al. Oncology nurses’ experiences of providing emotional support for cancer patients: a qualitative study. BMC Nurs. 2024;23(1):58. doi: 10.1186/s12912-024-01718-1.
38 Ichihara K, Nishiyama C, Kiyohara K, Morita T, Tamura K. Nursing care for spiritual pain in terminal cancer patients: a non-randomized controlled trial. J Pain Symptom Manage. 2024;67(2):126-137. doi:10.1016/j.jpainsymman.2023.10.016.
39 Anshasi HA, Fawaz M, Aljawarneh YM, Alkhawaldeh JFM. Exploring nurses’ experiences of providing spiritual care to cancer patients: a qualitative study. BMC Nurs. 2024;23(1):207. doi:10.1186/s12912-024-01830-2.
Funding and Acknowledgments:
This research received no external funding.
Conflict of Interest Statement
Nothing to declare.
Data Availability Statement
No databases were generated in this study. The information presented is described in the body of the article.
Authorship criteria (author contributions):
Autor 1 - Renata da Silva Lopes. Contributions: Study conception and design, data analysis and interpretation, and final critical revision of the manuscript.
Autor 2 - Giovani Basso da Silva. Contributions: Study conception and design, data analysis and interpretation, and final revision of the manuscript.
Autor 3 - Paloma Rodrigues Spies. Contributions: Data analysis and interpretation.
Autor 4 - João Gabriel Toledo de Medeiros. Contributions: Final critical revision and intellectual review of the manuscript.
Autor 5 - Eliane Goldberg Rabin. Contributions: Study conception and design, and final critical revision and intellectual review of the manuscript.
Scientific Editor: Ítalo Arão Pereira Ribeiro. Orcid: https://orcid.org/0000-0003-0778-1447
Rev Enferm Atual In Derme 2026;100(2): e026059
![]()